 |
| |||||||
|
The Power to be your best
ternyata tak ku duga, di sini mulai cerita KRONOLOGIS KARYA » HEPATITIS A ± Resensi - Technologi © MIS. Posted : 2012-03-02 : 03:41:21 (4875 hari 00:21:31 lalu) HITS : 1562  () ()  RESENSI : Hepatitis A has an incubation period of about four weeks. The virus replicates in the liver. Relatively large quantities of virus are shed in the feces during the incubation period before the onset of clinical symptoms, and a brief viremia occurs. RESENSI : Hepatitis A has an incubation period of about four weeks. The virus replicates in the liver. Relatively large quantities of virus are shed in the feces during the incubation period before the onset of clinical symptoms, and a brief viremia occurs.
| ||||||||
 Outbreaks of jaundice have been frequently described for many centuries and the term infectious hepatitis was coined in 1912 to describe the epidemic form of the disease. Hepatitis A virus (HAV) is spread by the fecal-oral route and continues to be endemic throughout the world and hyperendemic in areas with poor standards of sanitation and hygiene. The seroprevalence of antibodies to HAV has declined since World War II in many countries, but large epidemics do occur. For example, an outbreak of hepatitis A associated with the consumption of clams in Shanghai in 1988 resulted in almost 300,000 cases.
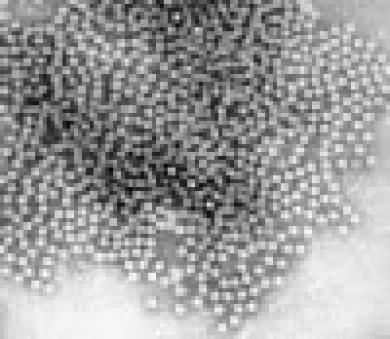
Outbreaks of jaundice have been frequently described for many centuries and the term infectious hepatitis was coined in 1912 to describe the epidemic form of the disease. Hepatitis A virus (HAV) is spread by the fecal-oral route and continues to be endemic throughout the world and hyperendemic in areas with poor standards of sanitation and hygiene. The seroprevalence of antibodies to HAV has declined since World War II in many countries, but large epidemics do occur. For example, an outbreak of hepatitis A associated with the consumption of clams in Shanghai in 1988 resulted in almost 300,000 cases.Hepatitis A has an incubation period of about four weeks. The virus replicates in the liver. Relatively large quantities of virus are shed in the feces during the incubation period before the onset of clinical symptoms, and a brief viremia occurs. The severity of illness ranges from the asymptomatic to anicteric or icteric hepatitis. The virus is non-cytopathic when grown in cell culture. Its pathogenicity in vivo, which involves necrosis of parenchymal cells and histiocytic periportal inflammation, may be mediated by cellular immune responses. By the time of onset of symptoms, excretion of virus in the feces has declined and may have ceased and anti-HAV IgM increases in titer. Anti-HAV IgG may be detected one to two weeks later and persists for years. Distinctive properties Electron microscopic examination of concentrates of filtered fecal extracts from patients during the early stages of infection reveals 27 nm icosahedral particles typical of the Picornaviridae (Figure 1). HAV was classified in 1983 in the genus Enterovirus (as enterovirus 72) of the family Picornaviridae, on the basis of its biophysical and biochemical characteristics, including stability at low pH. After the entire nucleotide sequence of the viral genome was determined, comparison with other picornavirus sequences revealed limited homology to the enteroviruses, and the virus is now considered as a separate genus, hepatovirus.  Figure 1,-- Figure 1,-- Hepatitis A virus particles found in fecal extracts by immunoelectron microscopy. Hepatitis A virus particles found in fecal extracts by immunoelectron microscopy. Both full and empty particles are present. The virus is 27 to 29 nm in diameter. (X 125,000.) The HAV genome comprises about 7,500 nucleotides (nt) of positive sense RNA which is polyadenylated at the 3′ end and has a polypeptide (VPg) attached to the 5′ end. A single, large open reading frame (ORF) occupies most of the genome and encodes a polyprotein with a theoretical molecular mass of Mr 252,000. The HAV polyprotein is processed to yield the structural (located at the amino-terminal end) and non-structural viral polypeptides. Many of the features of replication of the picornaviruses have been deduced from studies of prototype enteroviruses and rhinoviruses, in particular poliovirus type 1. Pathogenesis The clinical expression of infection with hepatitis A virus varies considerably, ranging from subclinical, anicteric, and mild illnesses in children to the full range of symptoms with jaundice in adults. The ratio of anicteric to icteric illnesses varies widely, both in individual cases and in outbreaks. Hepatitis A virus enters the body by ingestion and intestinal infection. The virus then spreads, probably by the bloodstream, to the liver, a target organ. Large numbers of virus particles are detectable in feces during the incubation period, beginning as early as 10–14 days after exposure and continuing, in general, until peak elevation of serum aminotransferases. Virus is also detected in feces early in the acute phase of illness, but relatively infrequently after the onset of clinical jaundice. Interestingly, antibody to hepatitis A virus that persists is also detectable late in the incubation period, coinciding approximately with the onset of biochemical evidence of liver damage. Hepatitis A antigen has been localized by immunofluorescence in the cytoplasm of hepatocytes after experimental transmission to chimpanzees. The antigen has not been found in any tissue other than the liver following intravenous inoculation. Pathological changes produced by hepatitis A appear exclusively in the liver. Several such changes occur: conspicuous focal activation of sinusoidal lining cells; accumulations of lymphocytes and more histiocytes in the parenchyma, often replacing hepatocytes lost by cytolytic necrosis predominantly in the periportal areas; occasional coagulative necrosis in the form of acidophilic bodies; and focal degeneration. Host Defenses Antibody to hepatitis A virus develops late in the incubation period. Specific hepatitis A IgM is found in the serum within 1 week from the onset of dark urine, reaching maximum levels after 1 week and declining slowly during the next 40–60 days. Specific IgG antibody appears shortly after IgM is detectable, reaching a maximum titer after 60–80 days. This antibody is protective and persists for many years. Epidemiology Viral hepatitis type A (previously named infectious or epidemic hepatitis) occurs endemically in all parts of the world, with frequent reports of minor and major outbreaks. The exact incidence is difficult to estimate because of the high proportion of subclinical infections and infections without jaundice, differences in surveillance, and differing patterns of disease. The degree of under reporting is believed to be very high. The incubation period of hepatitis A is 3–5 weeks, with a mean of 28 days. Subclinical and anicteric cases are common and, although the disease has in general a low mortality rate, patients may be incapacitated for many weeks. There is no evidence of progression to chronic liver damage. Hepatitis A virus is spread by the fecal-oral route, person-to-person contact; and under conditions of poor sanitation and overcrowding. Common source outbreaks are most frequently initiated by fecal contamination of water and food, but waterborne transmission is not a major factor in maintaining this infection in industrialized communities. On the other hand, many food-borne outbreaks have been reported. This can be attributed to the shedding of large quantities of virus in the feces during the incubation period of the illness in infected food handlers; the source of the outbreak often can be traced to uncooked food or food that has been handled after cooking. Although hepatitis A remains endemic and common in the developed countries, the infection occurs mainly in small clusters, often with only few identified cases. In 1973, immune electron microscopy led to the identification of virus particles in extracts of feces (Figure 2) during the early acute phase of illness, providing the long-awaited lead to further studies of this infection. Availability of viral antigen permitted, in turn, identification of specific antibody, development of serologic tests for hepatitis A, and determination of susceptibility to infection in human and nonhuman primates. Human hepatitis A has been transmitted to certain species of non-human primates shown to be free of homologous antibody, thereby providing a model for experimental infection and, initially, also a source of reagents. Figure 2. Immune aggregate of hepatitis A virus following the addition of convalescent serum to a fecal extract during the acute phase of the illness X 400,000 (from a series by Anthea Thornton and A J Zuckerman).  Figure 2.-- Immune aggregate of hepatitis A virus following the addition of convalescent serum to a fecal extract during the acute phase of the illness X 400,000 (from a series by Anthea Thornton and (more...) Figure 2.-- Immune aggregate of hepatitis A virus following the addition of convalescent serum to a fecal extract during the acute phase of the illness X 400,000 (from a series by Anthea Thornton and (more...)The availability of specific serologic tests for hepatitis A made possible the study of the incidence and distribution of hepatitis A in various countries. These studies have shown that infections with hepatitis A virus are widespread and endemic in all parts of the world, chronic excretion of hepatitis A virus does not occur, the infection is rarely transmitted by blood transfusion, and no evidence of progression to chronic liver disease has been found. Diagnosis Various serologic tests are available for hepatitis A, including immune electron microscopy, complement-fixation, immune adherence hemagglutination, radioimmunoassay, and enzyme immunoassay. Immune adherence hemagglutination, which had been widely used, is moderately specific and sensitive. Several methods of radioimmunoassay have been described; of these, a solid-phase type of assay is particularly convenient, very sensitive, and specific. Very sensitive enzyme immunoassay techniques are used widely. Only one serotype of hepatitis A virus has been identified in volunteers infected experimentally with the MS-1 strain of hepatitis A, in patients from different outbreaks of hepatitis in different geographic regions, and in random cases of hepatitis A. Isolation of virus in tissue culture requires prolonged adaptation and it is, therefore, not suitable for diagnosis. Control and Prevention of Hepatitis A In areas of high prevalence, most children are infected early in life and such infections are generally asymptomatic. Infections acquired later in life are of increasing clinical severity. Less than 10% of cases of acute hepatitis A in children up to the age of six are icteric, but this increases to 40–50% in the 6–14 age group and to 70–80% in adults. Of 115,551 cases of hepatitis A in the USA between 1983 and 1987, only 9% of the cases, but more than 70% of the fatalities, were in those aged over 49. It is important, therefore, to protect those at risk because of personal contact with infected individuals or because of travel to a highly endemic area. Other groups at risk of hepatitis A infection include staff and residents of institutions for the mentally handicapped, day care centers for children, sexually active male homosexuals, intravenous drug abusers, sewage workers, certain groups of health care workers such as medical students on elective studies in countries where hepatitis A is common, military personnel, and certain low socio-economic groups in defined community settings. Patients with chronic liver disease, especially if visiting an endemic area, should be immunized against hepatitis A. In some developing countries, the incidence of clinical hepatitis A is increasing as improvements in socio-economic conditions result in infection later in life, and strategies for immunization are yet to be developed and agreed. Passive protection may be obtained by the administration of pooled normal human immunoglobulin, containing at least 100 IU/ml of anti-HAV given intramuscularly at a dose of 2 IU/kg body weight. Post-exposure prophylaxis, if given early enough, may prevent or attenuate a clinical illness. Inactivated hepatitis A vaccines have been developed over the past decade and are now licensed in many countries. The virus grows poorly in cell culture but yields have been improved by adaptation and are sufficient to permit gradient purification. This virus is inactivated with formaldehyde and the antigen adsorbed to aluminum hydroxide and given intramuscularly. The preparations are safe and highly immunogenic in man and have been shown to induce a protective immune response in susceptible non-human primates and during extensive clinical trials in man. Attenuated strains of HAV have been developed and may be useful potentially as vaccines. This approach is attractive because live vaccines are cheaper to produce and tend to mimic the antibody response induced by natural infection. As with vaccine strains of polioviruses, attenuation may be associated with mutations in the 5′ non-coding region of the genome which affect secondary structure. There is also evidence that mutations in the region of the genome encoding the non-structural polypeptides may be important for adaptation to cell culture and attenuation. However, markers of attenuation of HAV have not been identified. Excretion in feces occurs and reversion to virulence may also be a problem. On the other hand, there is also concern that “over-attenuated” viruses may not be sufficiently immunogenic.   Jawa, 2012-03-02 : 03:41:21 Salam Hormat MIS Mutiara Sukma MIS Mutiara Sukma mulai gabung sejak tepatnya Minggu, 2011-04-24 21:23:51. MIS Mutiara Sukma dilahirkan di Bandung mempunyai motto Jadikan diri sebagai haadiah bagi kebaikan untuk sesama. Berita : 242 Karya Resensi : 30 Karya Opini : 33 Karya Puisi : 81 Karya Cerita Pendek : 6 Karya Sejarah : 2 Karya Cerita Bersambung : 3 Karya Laporan : 15 Karya Prosa : 3 Karya Biografi : 12 Karya Wacana : 2 Karya Filsafat : 48 Karya Kisah Nyata khusus Privacy : 4 Karya Pantun : 1 Karya : 4 Karya Lyrict : 1 Karya Surat dari Hati : 68 Karya Kisah Nyata non Privacy : 1 Karya Total : 556 Karya Tulis DAFTAR KARYA TULIS MIS Mutiara Sukma
Isi Komentar Hepatitis A 3450 ATAU berikan Komentar mu untuk karya Hepatitis A 3450 di Facebook
Terimakasih KASTIL CINTA KU , CORNER KASTIL CINTAKU Mutiara Sukma Kemarin tinggal sejarah. Esok hanya sebuah fatamorgana. Hari ini adalah nyata. MIS Mutiara Sukma : Dian Tandri | Suryantie | Ade Suryani | Arum Banjar Sarie | Ambar Wati Suci | Chintia Nur Cahyanti | ||